Okay. So here we are with another session At The Board. I’m really happy to see all of you out there. Now today’s going to be a topic – it’s going to be just a little narrow focus on lingual root, the palatal root of maxillary bicuspids. Usually that would be the first bicuspids. So the reason I’m doing this is because I have gotten some conversations from you out there, especially some of you RUDDLE+ people, and you’re going when are you going to talk about that lingual root? It’s so far into the palatal we thought it was harder than the palatal root of a maxillary molar.
So I want to just have a brief interruption of what I really normally wanted to do, and just give you a little heads-up on that area so some of you can be more comfortable when you’re assessing maxillary first bicuspids for surgery.
All right. I want to thank you for joining us again, and I want to thank you for all the activities and questions that are coming in. A lot of you are signing up and you’re getting baptized regarding surgery. We have these big continuums, as you know, and we’re not releasing intentionally everything at once. Because by the time we get to the end, I might even have to go back and edit something if conditions on the ground change.
But just understand that we’re releasing at a cadence. We’re about a dozen in on surgery, and we have to get to almost 30. So there’s a lot of content that lies just ahead. Let’s get started.
All right. So the palatal root, the lingual root; it’s the same difference. But let’s look at the challenges. When you assess this tooth, I think you would immediately think we’re not doing retreatment because there’s too many violations of the cleaning and shaping objectives. The mechanical objectives, we can just rattle them off real quick; we’ll reduce it to four. Look at any canal and ask yourself, is there a continuous, tapering preparation?
Maybe we should do it a little bit different. Maybe we should look at the other angle and come even more mesial so you can see those canals more in their entirety. So do we have a continuous tapering preparation? That’s a yes or no; you’re the clinician, you’re assessing, retreatment or surgery.
Did we maintain the original anatomy? It’s hard to imagine; you could have all this going on up here and that foramen was kept really nice and tight in its physiologic dimensions. Did we maintain the position of the foramen on the external root surface, and did we keep the foramen as small as practical? So when you start to click through these objectives, you start to realize we have no chance of retaining this. In fact, I’m going to come back and say I’m not showing you intentionally; I had the third angle.
We always want to get three horizontally angulated films. We can come straight on, break the contact areas, we can do that. We see the cull; you can see the cull area in here, you can do all that. But when we start to move the cone more anterior, we get to see that buccal root moving off towards the posterior. And that frees it up so you can really assess.
Now you might have liked your – the lingual root, continuous tapering preparation, the original anatomy, maintain the original anatomy, maintain the position of the foramen maybe, and keep it as small as practical. As small as practical; I didn’t say possible, I said practical. Maybe -- maybe on the lingual; maybe on the lingual. But not so much on the buccal. On the buccal we have a lot of violations of the mechanical objectives.
The more mesially angulated film also starts to throw the roots around, and it starts to give you a sense of what lies ahead. In other words – look at my fingers – are the roots like this? This is your x-ray, right? You say well I don’t see barely one root, but maybe I see now two. Are the roots in a proximal view like this? Or is there significant splay? Is there significant splay where these roots are really being thrown further and further apart, in mesially, progressively angulated films? So get one and then come mesial to mesial; okay?
And as long as you’re using your aiming devices, your Rinn kit devices, you’re going to get pretty good images, one-to-one, but it’ll help you diagnostically. The endodontists are screaming; they’re yelling Cliff – CBCT! Well you don’t all have CBCT, but if you had that, yes; if you have tomosynthesis, check that box as well. Look at image stacks like we’ve talked about in previous shows.
So you begin to plan your surgery because you realize you can throw these roots quite a bit apart and you know the distance. You’re going to raise a flap up; you’re going to lift this flap up and free it up here. And then you’re going to make your access and you’re going to come through here, and you’re going to have to take a lot of that buccal root off. You’re going to have to lose at least about one-third of the overall length.
So this brings us back to periodontal probing, mobility, crown/root ratios, is this the best treatment approach, should we do an implant, could we do a bridge, what should we do? So if you start to think like that you’ll have the right answer.
So understand then about one-third, the apical one-third of that buccal root is going to be gone, because you need access, access, access. It’s just like occlusal access. You can make a really small ninja access, okay? Can you find all the orifices, can you visualize the axial walls, can you see fractures? If you can do all that, you can make them as small as you like.
And then of course that’ll get us on over to the lingual root, the palatal root. So I’m referring to this as lingual or palatal, for international guests the same thing, same difference. But we’re going to have to get to that root as well.
So with all your imaging, whether it be CBCT, tomosynthesis, conventional radiographs, three different horizontally angulated films; get them. And treatment plan for no surprises, how about that?
Okay. Now that we have that out of the way, let’s come back to the case and show it. So when I made the flap and lifted the flap up, you immediately see – we’re looking at about right in here; right in here. The gutta-percha is leaving the root laterally, and it has perforated laterally, and the apical extent of the cone is lying right up over the root. So it’s superimposed over the root, and I’m pretty close to the board, but you might say it actually looks like it’s inside the root. Maybe in some dimension. So you might have been a little fooled on that; CBCT would have plucked that right off. But remember, that just has come on really strong in the last 10 years, 15 years, and it only arrived in the United States in 2001. So it’s still, we would say, relatively new technology about a quarter of a century in. Because so few of you have it.
All right. So that is a perforated root, so we’ll start to work on that. And as we knock that root down, as we knock that root down, just like we said, it’s nice and flat, it’s been almost a zero-degree bevel, and you can see it probably – I’m again close to the board, but maybe you can sort of see it if I go like that. And you might even see the foramen right in there. So all that to get across to see the apical one-third, to see the big old dome-shaped palatal root from the buccal view, and to get a good visualization.
So go ahead and begin to knock that down so the apisection continues so you have nice flat tables. You can use methylene blue and dye, make sure you’re around the root and you can read PDL; the dye will be absorbed into the periodontal ligament space. And I’m using, back in that day, one of the first ones in the world, we were using coated surgical ultrasonic instruments. Thank you Gary Carr for getting the concept going. You didn’t do the coated part and the contra angle part, but you certainly gave us the root end preparation idea. Then others came behind and made the instruments even better and more efficient. And less wedging because we could cut with easier motions with a coated instrument.
So we also had tips that were 3mm long, and we had tips that were 5mm long. So we could go further up the long axis, but then you had to have enough room in here to introduce the instrument. So you might have to start with a 3, and that would be a little smaller profile; and then once you get that prepped out down in deep, then you can come in with a 5. And a 5 might be able to not quite hit here, and I’m not saying remove more bone; I’m just saying you can start to usher it into the prep and then stand up your handpiece and you’ll be able to go 5. So that’s just a little idea.
And so very quickly we’ll walk through it. There’s the two roots; you can see they’re stair-stepped just like we showed. Look at all this height in here; we’re saving that root. A lot of times I see clinicians knock the roots down so they’re kind of on the same plane, but you’re going to really shorten the stability of that tooth by shortening – by needlessly shortening the lingual palatal root. So that’s that dimension, you can see it right there.
I pride myself in photography. It wasn’t so easy, and a lot of these were done before video was even remotely good. And certainly you couldn’t get grabs off of video to have a really sharp resolution; an image with a good resolution. So that’s our retro preps, and you can see them quite nicely. But to really look up the prep, and to really evaluate; do you have gutta-percha left on your axial walls of the prep? Is there any debris residual to the prep? Are you on the long axis, or did you get a little bit deviant? This is a way with these tiny retro mirrors that we talked about decades ago. And in the surgical symposium on RUDDLE+, you can see a lot of things we did with the mirrors and how we used them in a lot of just routine, bread and butter surgeries. But to me, I love to evaluate. A lot of people prep, but come out, and it’s a blind shot to go right on and fill. Why not evaluate it? Why not evaluate it?
And why not even use the little mirrors to look at your seal? Whether you used MTA, whether you’re using amalgam, super EBA, whether you’re using some kind of a bio ceramic putty. Okay, that’s fine, that’s all good. Whatever you’re using, evaluate the cork.
So we started with that. We’ve shortened those roots down as you just saw surgically; got quite a bit more height up here on this root as compared to the buccal root. And you can begin to see if you watch with time, the bone comes back in. Endodontics properly performed is a regenerative procedure; it sets the stage for ossification, bone growth, reattachment, and that’s what makes endodontics the foundation of restorative and reconstructive dentistry.
So that’s just one case, and now we’ll move very quickly because I showed you kind of the nuts and bolts. Now you’ll need to go to RUDDLE+ is you want to know all the things about flaps, elevations, crypt control, hemostasis, apicoectomy, retro preps, suturing. Okay, all that’s somewhere else. This was just I’ve had some issues lately with people calling and saying oh that lingual root’s deep. You know what? It is deep. It’s one of the hardest surgeries in the mouth. The palatal root of the molars, the lingual or palatal root of the first bicuspids. And of course there’s some issues down below; mandibular canal, middle foramen, and then the inclination of incisors. All of that’s discussed in another venue and in more content.
So now that you’ve see this, and I’m so close to the board today for some reason, I can’t see my own work. But this was done recently by and endodontist in southern California, within six months. They’ve been on an antibiotic post treatment. This tooth was percussion positive and palpation positive. But if we apply that to this tooth over here, this one, it was percussion – boom, boom, boom. In other words you couldn’t even touch the tooth. That tooth was very, very sore in palpation; there might have even been a little fullness up in the vestibule. And the roots were very, very close to the cortical plate. In fact, I wonder if I had CBCT in that era if I would have lifted the flap the root would have been right there; because you could feel that. So don’t forget to palpate; it’s one if the most important things. Because if you kind of feel the prominence of the root – here’s the gum over the finger; if you’re out here and you can kind of feel that prominence, you know that root’s right there.
Well now let’s come back and look at that root. In other words, Ruddle’s a big advocate of disassembly and non-surgical retreatment. That’s what I do for myself. But when we can’t be successful, then we have to have another idea; and it’s either extraction, implant or bridge.
But look at this root; let’s look carefully together. I’m reading it as coming up like this, coming around like that; I see the PDL here coming around like that. This root should have curved and gone over like that. But it was first, I imagine, blocked. What do we know? We’ve already talked about this in other shows. The block invites the what? And what happens if we keep working on the outer wall? We get a perforation.
So I believe the lingual root was blocked, ledged and perfed. But the packing is pretty remarkable. We get hydraulics; I see a portal of exit. You know, some people say these are sexy, the lateral canals. It’s not the lateral canals that are sexy; it’s the portals of exit that need to be sealed.
So this person got quite a bit of hydraulics, because I see something here. The cone ended there, and I called the other endodontist and he said he could never get to the end of the root; he was very frustrated when he packed it. And he said geez, I drove some sealer and got a little squig. So you know, that’s happened to Ruddle. And this one I don’t think I could ever kick my files back in the physiologic canal. So when I told this to the patient and the referral, we all agreed. We’ll just lift the flap and it might be two teeth. We’ll start off with the obvious one, the one that I identified was super, super sore to percussion; just light tapping, no banging with your mirror handle. So let’s go for it.
So we’ll go in there quickly. But you can see already there’s a lot of splay in these roots; I’m just showing you one angle. I could show you another angle where the buccal roots are over here, so now you know this is about a mile. Did I say a mile? I meant to say a kilometer; sorry. But the distance is quite remarkable from this root over to this root. And that’s what I’m talking about today -- challenges accessing the palatal root of maxillary first bicuspids. And I don’t have to show you a hundred. Just show you a couple and you’ll go okay, I get it. The next time I’m evaluating that tooth for surgery, or I’m going to refer it for an evaluation for surgery, I’m going to lose quite a bit of that buccal root and I’m going to make a long tunnel over there to the palatal. And I hope I have my microscope and I hope I have ideas, and I hope I can do a bloodless surgery so I can see.
So anyway, the other thing you notice is it’s up a lot higher on another plane. This one’s beveled down on this plane. This one’s beveled up here and it’s on another whole plane. So that’s how we keep root length.
Now one thing I noticed when I was doing this is I had to put quite a bit of ferric sulphate; ferric sulphate. Because I was getting a lot of bleeding. And when I was all done here, I just kind of punched through and copious amounts of bleeding. So I realized, where’s all the blood coming from? There’s no important anatomy right there. It must be granulation tissue, and granulation tissue has a profuse abundance of capillary beds; it bleeds, it’s the first tissue in disease, it’s the first tissue in wound healing. So I decided we’re here; let’s just move over. Made a separate crypt, made another hole over here, and went ahead and got the other tooth. And there we are.
So we were using the 5mm length retro instruments so we could get further up the canal, corked it nice. And you can see that if we just let a little time intervene, the bone has grown back marvelously around all the roots. You can see the PDLs coming in beautifully, and that’s endodontics.
So when we have little errors of omission, and when we have little problems sometimes because we’re not patent and we’re in a hurry and we lose our focus, sometimes we have to take those cases. Because there’s now no way we’re going to undo what we did. We can’t put the dentin back, so now we have to go think of another way. And surgery could be the approach with just – again, recognize when you start to see divergence, you start to do – whatever religion it is, you do something to help you along.
And this will be the last case. And again, it’s tied up in an extensive amount of dentistry; the costs, the stakes are high. I talked about of course, if you know Ruddle the consultation involved talking about accessing through the bridge abutment. It’s double abutted; you can’t see that, but I’ll do it like that. It’s double abutted, so it’s a 1,2,3,4-unit bridge.
But notice we have posts. They’re not long posts; they’re not threatening. This is paste, that’s not gutta-percha. Is it brick-hard paste, does it have some kind of a cortical material to keep it soft? These are things we don’t know and we can’t get the history on it.
So after weighing all that, the patient said well can you just leave everything alone? Because I have like $1200, $2400, $4800; I have about $5000 worth of dentistry invested, and that way we won’t touch it. So we said fine; we’ll go in the other way.
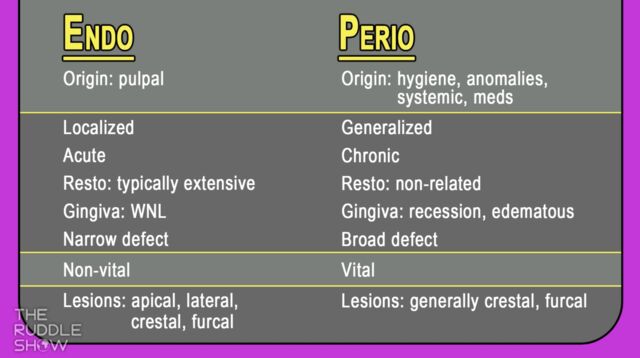
The lesion looks to be apically. I don’t see a component laterally; I don’t see an infrabony pocket where we could have a POE feeding that. These are all things we’ll talk about when we get more into endo/perio, perio/endo. Is it a lesion of periodontal origin, is it a lesion of endodontic origin? Those are all things we’re going to want to know.
And we’ve talked about that, right, so you already have a little clue on that. But what I can see after our discussions from today earlier, we need to do about probably 5,6,7 hours and we’ll add a show on the continuum where we’ll talk about all the things than encompass that.
So end to this case. I wanted to trace the sinus track. There was fornix of the vestibule, there was a sinus track, and we can trim off the non-useful end of the gutta-percha cone and slide it back in there and take another film. It looks like a mistle from 50 yards. I just watched the Olympics; it might be a piece of a javelin. All right. Everybody’s serious, so maybe you can smile just a little bit out there. Maybe you’ll feel just a little better if you smile. Smile; the world’s going nice.
So you cut right to the chase. Again I like these little longer preps. You’re noticing some can be 3mm, some can be 5mm. But the more space we eliminate as being a source of potential infection to the attachment apparatus, the more successful our results.
So I think we have a healing case shot in here, and there it is. So look at how our lesion appears to be kind of like this; you saw me trace it with a gutta-percha cone. And now you can see how tight the bone is. And again, properly performed endodontics is the cornerstone of restorative and reconstructive dentistry.
I hope you’ve enjoyed the approaches to the posterior roots, and I’ll leave you with one last comment. Because the lingual root, the palatal root is so far to the lingual, be sure you measure twice because you can only cut once.