Hello everyone. My name is Reid Pullen. I’m an endodontist in Southern California. I’ve been an endodontist for 18 years in clinical practice; it’s call Brea Endodontics. I’d like to say it is a huge honor to be on The Ruddle Show, Cliff Ruddle; thanks for inviting me. I want to say that I was a general dentist for five years -- three years in the military and then two years in private practice. I had an inkling that I wanted to be an endodontist, and so I came to this lecture in Anaheim at Disneyland by this famous endodontist named Cliff Ruddle. And I watched him lecture for the day and that was it.
After I heard Cliff Ruddle speak, I said I’m going to be an endodontist. I was set, and I am so grateful for that lecture and for your mentorship, even as a general dentist through your lecturing. And then as I became an endodontist, you helped; you mentored me throughout those times, and you helped me become a better person and a better endodontist. So thank you so much for that, and let’s get into the presentation.
I want to talk today about something called – I call it the Super Slider; or the Sexy Slider. This is a new paradigm in endodontics, because this file will make you so efficient, so effective, and help you get an excellent result. So we’re going to talk specifically about one NiTi file called The Slider.
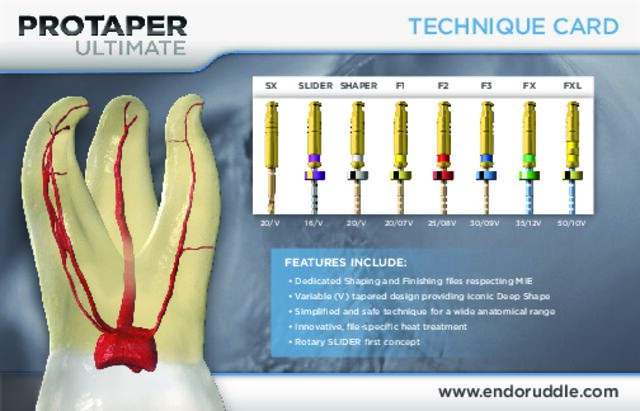
Now this comes from the ProTaper Ultimate instrument family, and this is The Slider; this is what we’re going to focus on. The ProTaper Ultimate is kind of a new instrument system that is the evolution of ProTaper Gold. So basically Cliff Ruddle, John West, Pierre Machtou, as you know from The Ruddle Show, they took ProTaper Gold and they made it a little bit smaller from 1.2mm diameter to 1mm diameter. And they wanted to focus on a minimally invasive type shape, and so that’s how the ProTaper Ultimate family came into existence.
But they created a Slider, and I want to talk about the Slider because it is really an exciting file. Here it is, the Super Slider, and it’s something we call a rotary negotiator. And this is kind of a new concept in endo. We were always taught as students in dental school, and even as we got out and even in the residencies, endo residencies, to always use a hand file to negotiate down the canal. Well, in this file system, ProTaper Ultimate, the Slider actually replaces the hand file; okay, most of the time – I’ll talk about that. You can use the Slider as your rotary negotiator, and it’ll advance down the canal to working length, through the apical minor constriction to patency. And you can actually negotiate to patency and get a working length and a glide path in just seconds.
Now, the cool thing with the Slider is I use it – I use a Slider; with any file system that I use, I start with the Slider. So obviously, ProTaper Ultimate is a great system; I’ll use the ProTaper Ultimate. I also love ProTaper Gold and WaveOne Gold. But any of those file systems that I’m using, I will start with the Slider and I will use that as my rotary negotiator.
So here is just kind of a look at the ProTaper Ultimate, and specifically the Slider, which is made of M-Wire, so it’s a little more resistant to cyclic fatigue – it’s a heat-treated file system. And when you look at the dimensions of the Slider, you can see it’s got a 16th tip size, so that’s perfect. Basically, a glide path is when you at least get a 15-hand file down to working length; and that’s kind of our goal to get an open glide path. This satisfies that by having a 16th size tip and a 2% taper at the tip.
You want to run this at 400 rpms and 4-5.2 Ncm torque, okay? A little bit different than the 300 rpms that you run ProTaper gold, or 500 rpms if you’re using Vortex Blue. This is 400 rpms and you’re using the 4-5.2 Ncms on the torque. You’re going to use very light pressure; especially with the Slider. Remember, you’re using – you’re asking this to negotiate down the canal where no file has been before. So this is a file that’s advancing; you want to use very passive hands when you’re using the Slider.
I always start – I find the canals first; easier said than done on some cases, right? I find all the canals, and I always start with a coronal negotiation with a 10C shorty. In fact, this is I think the tip of the day, right here. Every time you find a canal, always explore that coronal third with a 10C, 21mm file. The C-file is a little stiffer than a K-file; the 21mm file is shorter than a 25. Dip it into RC Prep and get in there and explore each canal; and just make sure that it’s open in the coronal third. Make sure that there’s not any calcification, or that a pulp stone fell into one of the canals. Just make sure it’s nice and open, nice and smooth, about 10 or so millimeters down; then you can go in with your Super Slider and you can start to do your rotary negotiation. So I always start with my 10C shorty; make sure I’ve got a nice open canal in the coronal third.
Then I go in with my Slider. I say it’s the first file in; I mean it’s the first rotary file in the canal, and this is really the workhorse. Now what do I mean by that? I’m going to explain; I’m going to show you why I call this file the workhorse.
All right. So remember, we’re using this file instead of the 10K hand file or C file to negotiate the patency; to negotiate down to working length. So before they put this file out, they wanted to test it. And so Dentsply Sirona sent this file system out to a bunch of endodontists. They tested it; they came up with 63% of the time, this group of endodontists were able to get down to working length, down to the apex with the Slider, without using hand files; 63% of the time, okay?
So I wanted to do my own little tests because when I started using it, I was getting pretty good results. So I wanted to see if that number held true, or was it lower or higher; but I was getting pretty good results. So I went ahead and started testing this. I’ve been testing this for over a year; I’m at 1,169 canals, and I am at an 80.5% success rate. Okay, this is pretty killer. Because as an endodontist, I’m treating some very difficult cases. 80.5% of the time, I can get this Slider to reach working length, without the use of a hand file, within one to three passes. Sometimes the first pass it won’t advance down to working length; it might take two passes or three passes. But a lot of times I’m able to get – 80.5% of the time – get down to working length without the use of a hand file. And this is brilliant when I do this; it makes the treatment so fast. This is where I reached the apex passively.
Now, what are the benefits? Why is this the workhorse and what are the benefits of using the Super Slider? Well, step one. 80.5% of the time you’re able to negotiate to patency, efficiently and effortlessly. It just slides right down the canal to the end, pops out the minor constriction, and you can then get in an accurate working length by hooking up your apex locator right to the Slider. You can slide it to the Slider shank or to the handle; doesn’t matter. You can get a nice, accurate reading.
Third, it will cut a nice, open glide path. So you’ll be able to negotiate to patency, achieve an accurate working length, and achieve an open glide path in seconds. Sometimes on a simple to medium difficult case, I can do this in three canals in less than 30 seconds. And it just makes your life easy. It’s simple because you’re able to get a nice, quick working length, cut an open glide path. You negotiate it down, you get a nice working length, and you cut an open glide path; and then you’re ready to shape. And the shaping then is easy.
The hard part is all the stuff before the shaping; finding the canals and then getting down the canals. That’s the hard part. If you can do this; if you can find a file that can help push you to be better and to do this faster and safely, then that’s the bonus, and that’s where the Super Slider comes in.
Okay, so what about this 20% of the time? I’m successful 80.5%; what about 20%? What happens then? So sometimes you put the Slider in and it’s hitting a brick wall. It just won’t go around – it’s usually a little apical curve. It just won’t go around that apical curve, and you go bam! You feel it hitting a brick wall. Hitting a brick. Once you do this, just forget it. Take it out, take the Slider out; take a deep breath and go traditional. Negotiate to patency with either an 8 or a 10K file. What I typically do is I’ll put a little 45° apical curve or bend of that 8 or 10K file, dip into RC Prep, and I’ll go in there and I’ll take it on a walk around the apex. I’ll take it on a walk around, trying to find where that little curve is; that apical curve. So no big deal. If it doesn’t work 20% of the time, you just do a traditional hand file. You get working – you get patency, then you get working length, then you’ll do a glide path – an open glide path. Okay, so that’s what happens 20% of the time.
Now what about the dark side; the dark side of using rotary negotiation? That would be file separation. Okay, so it can happen. If you don’t have – if you’re rough with this, you can separate. Now I’ve separated – you saw how many canals I did. I did over 1000 canals; over 1100 canals; I’ve separated three times. Now two of them were early and one was recent. I was being a little bit rough. All three of them I was being rough; two of them I was able to bypass. One of them I got stuck; it was stuck at the end, done. No big deal; a lot of times it will still work. It’s not pretty. We don’t want that. But it’s very rare. And if you use passive hands – which I’m going to show you right now – you can prevent this. If you feel like the Slider is hitting a brick wall, you stop, you pull it out, and you go traditional hand files to negotiate to patency. Okay?
So here’s the feel. You almost hold the file; it’s passive. It’s just a passive feel. You barely – you’re not pushing on the file; you’re letting the file kind of just lead you in there, lead you down the canal. So you hold it with very light pressure; you always dip the tip of the Slider with RC Prep or ProLube. This is the only NiTi file that I dip. I don’t dip my files; I’m not a dipper. I only dip the Slider with RC Prep, because I’m asking it to negotiate down to patency where no file has been before. So it’s doing – it has to kind of rip through that tissue; I want a little bit of lube in there to help it do that so it doesn’t get caught up.
The key is, when you’re using the Slider, don’t be a construction worker. Don’t hammer this Slider into the canal when it’s not going. If you’re hitting a brick wall, don’t hammer it like a nail; I want you to do your Zen endo. Take a deep breath, breathe through your nose, and very light pressure with this baby. Use your Zen endo when you’re using the Slider. If it’s not advancing to working length, then get out; get out and use hand files. But again, 80% of the time it’s going to go down to working length within 1-3 passes; so it’s really a beautiful, beautiful thing.
Here is the Slider dipped with RC Prep; I’ve got the dip. Dip the tip in there. Use your file lubricant. You can use Glide or ProLube or whatever you want, doesn’t matter, just use file lubricant.
And now I’m going to show you a video of a mesial buccal canal of an upper molar. Hard to get in there, to get that into the MB canal. I don’t have a coronal flare yet; I don’t do a coronal flare when I use this. I’m going to do the MB canal; I’m going to put a little teeny bend on it, just enough. Dip it into RC Prep, and then have the patient open a little bigger. Tooth #3 and there it goes; there we go. Got in there and now I can run it and see if it will run down to my estimated working length.
So let’s look at it; let’s watch this now. There we go. Now, I’m running it, nice easy, engage, disengage, nice and smooth, passive hands. I got down to my estimated working length. Hook up the apex locator – look, I’m long. I’m long, I’m long, I’m long. Perfect, right there. Push the stopper down, get your working length. That’s excellent right there. I just negotiated patency, obtained an accurate working length at 19.5mm, and I cut an open glide path in the MB canal of #3 in seconds. Boom! I just took away three big pillars of endodontics; three big pillars of endodontics in seconds. Negotiated patency, accurate working length, and an open glide path. So this is beautiful.
I would wipe the file; I would just go right into the DB canal. So I do it sequentially. MB canal, get my working length, go to the DB canal, then I go to the palatal canal; so I do it one after the other. In some cases in under a minute, I’ve got three working lengths, three glide paths that are open, ready to shape – the shaping is easy. The shaping is the easy part now. Finding the canals and getting down the canals is the hard part. So there we go; that was our working length.
Let’s look at a case – this is tooth #16, or #28 if you’re international. Tooth #16, very difficult case to treat. It’s a wisdom tooth, it’s infected. Let’s take a look at the CBCT. So here’s our cone beam. You can see the palatal canal in the MB 1; you can kind of see an MB 2 in there, vaguely. That’s the coronal view right there, the coronal view. Here’s sagittal view; you can see the palatal root. You can see there is a mucositis of odontogenic origin, because we have a periapical radiolucency on all three roots really; the palatal root and mesial buccal root, it shows here.
But then you look at the axial view and you can see that, unfortunately, there are four canals in this thing. MB 1, you can see the MB 2, you can see the DB and you can see the palatal. So I said shoot! This was an older individual, #16, four canals infected. I go dang it; I had some anxiety before I treated this case. But what happened, what I found was the Slider and the Ultimate, ProTaper Ultimate system, made it so easy and so fast to treat this, that I walked out of there just in awe of how simple it was to treat.
So I’m going to show you the MB canal, just showing you how I was able to get working length on this case. There’s my Slider; dip it into RC Prep or Glide or whatever you want. Get some lube in there. Let’s go to the MB canal. Now passive hands; in and out. Engage; disengage. Many in and outs. Nice and gentle; nice and smooth. There we go. That just walked – that Slider went right down to working length. Just hook it right to the handle; that’s your apex locator. Boom, got it! I was able to get working length. I was then able to get working length on all three of these canals. And then I later found the MB 2; had to work that one up too. I went up to a ProTaper Ultimate F2. But the Slider advanced to patency in all three canals, and it took me about a minute to get down each canal, to get a working length and cut an open glide path. So it was pretty cool.
Yeah, I finished this in a minute, and I was extremely happy with the result. Nice shape, nice cleanout. And I took a post op CBCT, just because I wanted to take a look at it. This is the coronal view here. And you can see the palatal root was perfect; MB 1 is good. The MB 2 is a little short on the fill, which I was slightly disappointed with myself. But let’s just – we won’t go crazy on that. Here’s the axial view. You can see how beautifully – how this minimally invasive file system, ProTaper Ultimate, cut these beautiful smaller shapes, and they stayed centered right in those roots so a really nice shape there. On the MB 2, I went to the F – I went to an F1, so I used a real small shape on that, on the MB 2. So that’s that; that’s the case.
Now, the last thing I want to talk about is I’ve been using the Slider. I use it with ProTaper Ultimate, or I’ll use it with ProTaper Gold, or I’ll use it with WaveOne Gold too. So I kind of hybridize it sometimes. The Slider is such a valuable file, because I’m able to negotiate to working length passively without the use of a hand file 80% of the time. So why not use it for every case that you do, even if you’re not going to use the Ultimate system? Which is a great system, but I’ve been doing this Slider Gold technique; or I call it the FAB technique because it’s just fast and beautiful. It’s such a great technique. It’s a hybridized technique.
I hesitated to talk about this; it can be a little confusing. But it’s just a hybridized technique where I start with the Slider, I do my rotary negotiation, get my working length, get an open glide path. Then what I do is I go to the ProTaper Gold Shaper 1. I leave it on the same RPMs, 400 RPMs, and I cut my middle flare. So I just run the ProTaper Gold Shaper 1 to working length; it cuts a middle flare. Then what I’ll do is I will finish the apical third with the WaveOne Gold Primary; and that’s that reciprocating file that reciprocates. And I will plus it. If you need to, this is just shape larger. If you need to go a little bit larger, WaveOne Gold medium, or you could cut with an F3, ProTaper Gold F3; if it’s a palatal root or a distal root that’s bigger, do that.
But most of the time, I’m finishing with the WaveOne Gold Primary. The reason this technique is so awesome, is because it is so fast. The rotary negotiation using the Slider, like I already said, on these simple to medium difficult cases, it takes less than a minute to get the Slider down to working length and to get your working length and glide path.
The ProTaper Gold S1, or Shaper 1, is one of my favorite files in the world. The Slider and the ProTaper Gold S1 are my two favorite files; I just love those. It just cuts a beautiful, balanced middle flare. I mean it just opens that middle third of the canal, and it gets it ready so you can just finish the apex. So I have probably shaped 10-15 thousand cases with ProTaper Gold; I just love that system. I love the WaveOne Gold system, and I love the ProTaper Ultimate system too for the smaller cases.
Then I come in and I quickly will shape the apical third using the WaveOne Gold Primary, which is a reciprocation. So you just have to change the setting one time and it’s crazy. This FAB technique, the Fast and Beautiful, gives you these fast and beautiful shapes. I call it also Fast as Bolt; FAB, Fast as Bolt. Usain Bolt, who has the world record in the 100 meter and 200-meter races in the Olympics. It’s that fast. It’s so fast, and you can just cut these shapes.
I want to show you an example of one. Here's tooth #15, or #27 in international speak. You can see the curves on this mesial buccal root; it’s got some curves. You can see the working length, it’s about 21; estimated working length is about 21. I was able to use the Slider Gold or the FAB technique. I used my Slider and my ProTaper Gold S1, and I followed up with the WaveOne Gold Primary. I shaped this case in like a couple minutes. And it was incredible. And I got a really nice, beautiful result; Fast and Beautiful, right? It’s just a very fast technique; very cool technique.
You cut and you can shape your canals fast, very efficiently. It gives you plenty of time for an activated irrigation. When you activate your irrigant, your sodium hypochlorite and your Q-Mix or your EDTA, you then get enhanced disinfection. And the easiest way to do this is by using the EndoActivator. The original EndoActivator on the left ran at 10,000 cycles per minute. The new EndoActivator runs almost twice as strong, 18,000 cycles per minute, and it is sonic activation at its finest. This is just a simple device to use to get a really clean canal. There’s lasers out there; the Light Walker Laser is good using SWEEPS technique. But they’re expensive, so some dentist don’t want to spend $100,000 on a laser. You’ve got this EndoActivator, especially this new one, 18,000 cycles per minute. You can get some beautiful cases with this. So if you can shape those canals fast, then you have plenty of time for enhanced disinfection, and to get the cleanest canals possible, and boom-boom; you got it.
Love to for you – a shameless plug for rootcanalacademy.com. Please go on the website; I’ve got lots of great instructional books, and they’re fun. I have a great time with these books; they really help you to be a better dentist when you’re doing root canal therapy. So please go see rootcanalacademy.com, right there. Love to see you; love to chat with you. And my favorite book is this WaveOne Gold. I’ve got six full cases; you get a QR code. Under the Microscope; you can watch my full cases where I’ve narrated them, and a step-by-step guide of how to do endo from start to finish. It’s one of my favorites, and it’s a surfing theme so lots of surfing in there too; pictures of my family surfing.
And then anyone interested in a two-day Root Camp Boot Camp, please go see rootcanalacademy.com. These are the dates coming up for this year; would love to see you. It’s a two-day course, wonderful course. I do a live patient demo, upper molar, and you can see that real clear.
So thank you so much. I’m really grateful to be able to share with you, and I hope I helped you. Always wanting to help you guys get better. If you need to get ahold of me, there is my email. Thank you so much, and you guys have a wonderful day. Thank you.